

Introduction
While 5-year event-free (EFS) and overall survival (OS) in Hodgkin lymphoma (HL) generally exceed 85% and 95%, respectively, outcomes may not be as favorable in adolescents and young adults (15 - 39 years [y]) compared to children. Small clinical trials have reported better outcomes for pediatric but not adult patients with mixed cellularity (MC) vs. nodular sclerosing (NS) histology, suggesting the possibility of biologic differences across the age-spectrum in HL. We examined survival by age and histology in patients receiving risk-based, response-adapted therapy for de novo HL on contemporary Children's Oncology Group (COG) trials.
Methods
This was a pooled analysis of individual-level data from 1,907 patients enrolled on three Phase 3 COG clinical trials for treatment of low-risk (AHOD0431), intermediate risk (AHOD0031) and high-risk (AHOD0831) HL between 2002 and 2012. Histologic subgroups included MC, NS and classical HL, not-otherwise-specified (cHL, NOS). Five-year cumulative incidence of relapse, EFS and OS were compared by age group (<15 y vs. ≥15 y) in the pooled cohort, and in histologic subgroups (MC and non-MC) using the Kaplan-Meier method. Effect modification was confirmed between age and histology. Cox proportional hazards regression models were used to examine the influence of age on EFS and OS, adjusted for race/ethnicity, Ann Arbor stage, B symptoms, bulky disease, receipt of radiation therapy (RT), and the interaction between age and histology; COG study was also included in the model, given that the criteria for response adaptation differed across the trials.
Results
Between 2002 and 2012, N= 2155 patients 1 - 21 y enrolled on three COG trials, 1,907 (88%) of whom were included in this analysis. Mean age of the cohort was 14.6 y (± 3.5) with N= 871 (46%) <15 y and N= 1,036 (54%) ≥15 y. In total, N= 1,547 patients (81%) had NS histology, N= 108 (6%) had cHL, NOS, and N= 196 (10%) had MC histology; by age, MC histology was present in N= 66 patients (7%) ≥15 y and N= 130 patients (15%) <15 y (p< 0.01). A significantly higher proportion of those ≥15 y vs. younger had B-symptoms at diagnosis (29% vs. 21%, p< 0.01), however the presence of bulky disease did not differ by age. Finally, patients ≥15 y (vs. <15 y) were significantly more likely to receive RT as part of their treatment (72% vs. 63%, p<0.01).
Survival: Median follow up was 6.9 years. In unadjusted analyses, 5-year EFS and OS were 83% and 97%, respectively. The 5-year EFS was lower for patients ≥15 y vs. <15 y (85% vs 89%, p<0.01), as was the 5-year OS (96% vs. 99%, p< 0.01). In multivariable models, age ≥15 y (vs. younger) was associated with a 1.4-fold increased risk of EFS (HR: 1.4, 95% CI: 1.1, 1.8, p< 0.01), and more than a 3-fold increased risk of death (OS: HR: 3.1, 95% CI: 1.5, 6.4, p< 0.01).
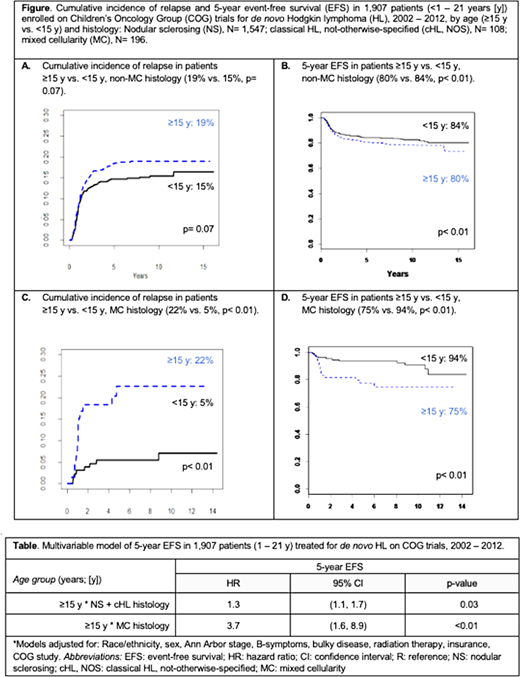
The effect of age on EFS varied by histologic subgroup. Among those with non-MC histology, cumulative incidence of relapse did not significantly differ by age in unadjusted models (Figure A), however 5-year EFS was significantly worse in the older group (Figure B). In multivariable analyses, age ≥15 y (vs. younger) was associated with a 1.3-fold increased risk of EFS (HR: 1.3; 1.03 - 1.7, p= 0.03) (Table). Among patients with MC histology, age ≥15 y (vs. younger) was associated with significantly higher relapse rate (22% vs. 5%, p< 0.01) (Figure C) and significantly worse 5-year EFS (75% vs. 94%, p< 0.01) (Figure D). This remained significant in multivariable models: patients with MC histology who were ≥15 y (vs. younger) had a 3.7-fold increased risk of EFS (HR: 3.7, 95% CI: 1.6, 8.9, p< 0.01) (Table).
Conclusion
In patients receiving response-adapted therapy for de novo HL on contemporary COG trials, adolescents ≥15 y had worse EFS and OS compared to younger groups. The magnitude of the effect of age was higher in patients with MC disease. Although recent pediatric trials in HL have indicated better survival for some children with MC histology, alternative approaches or novel therapies should be considered for older adolescents with MC disease, whose outcomes appear more like adults.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal